
This has been one of my most popular blog posts – I originally posted this as a 3 part series, which is still available in CompTalk.
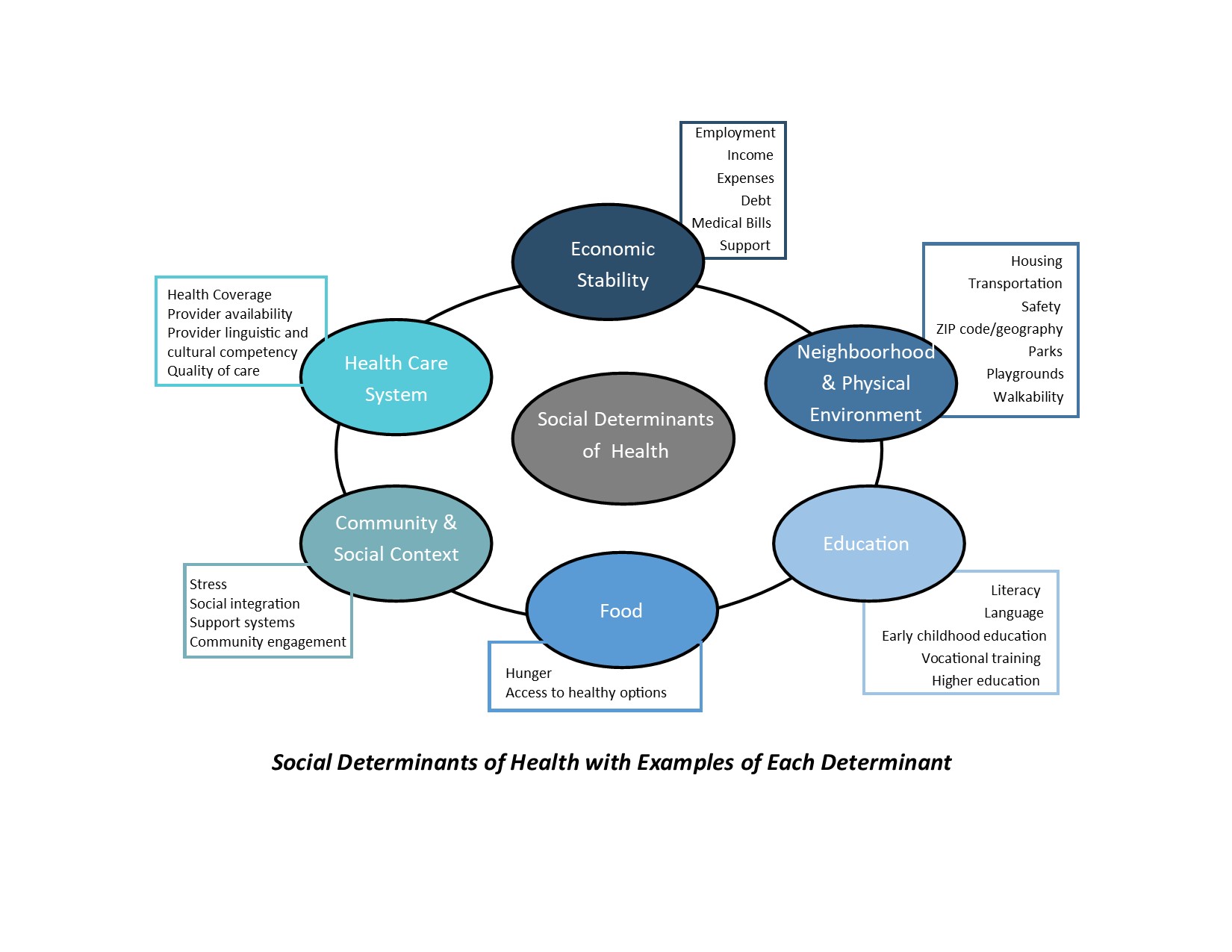
In the first part of this series I discussed the research on the impact of Social Determinants of Health (SDoH) and Adverse Childhood Experience (ACE) on the ability of our Recovering Workers (RW) to actively participate and adhere to their treatment plan post-injury, and the need to begin to utilize a Trauma-Informed Care (TIC) Model.
To review, a minority of workers with work-related injuries experience challenges returning to work. Early developmental trauma, including child abuse, neglect, violence persisting into adulthood, and drug misuse are only some of the examples of triggers that can create a sense of fear, helplessness, and overwhelm a person’s resources for coping, self-regulation, and perception of control, interpersonal relationships and self-efficacy.
In Part 2, I shared some of the available research that imbues the TIC model. In this re-visit to this topic, I was hoping we could all provide some insight into how we do, or should begin, to apply principles of Trauma Informed Care in the workers’ compensation industry.
The 3 E’s of Trauma
Include traumatic events, the individual’s experience of these events and the long-lasting adverse effects of the events. These may occur immediately or may have a delayed onset. The duration can be short to long term. These can be some of the non-work-related, preexisting conditions that can impact a successful return to work. In the workers’ compensation industry, we are just beginning to learn about SDOH and ACE, and the need to address these issues as they impact our RWs.
How do we Apply Trauma Informed Care in the Workers’ Compensation Industry?
As I tend to be a pragmatist, while I love to learn new things, I also like to think of how they apply, and how to use this knowledge to improve a process. I haven’t seen a lot of information on how this is to be accomplished within our industry. A solution I proposed in Part 1 was to provide TIC. The next question is HOW do we apply TIC in the workers’ compensation industry?
The 4 ‘R’s” are Key Assumptions in a Trauma-Informed Approach.
All people at all levels in an organization or system have a basic realization about trauma and understand how trauma can affect families, groups, organizations, and communities as well as individuals.
“A program, organization, or system that is trauma-informed realizes the widespread impact of trauma and understands potential paths for recovery; recognizes the signs and symptoms of trauma in clients, families, staff, and others involved with the system; and responds by fully integrating knowledge about trauma into policies, procedures, and practices, and seeks to actively resist re-traumatization.”
TIC involves understanding, anticipating and responding to the issues, expectations, and special needs that a person who has been victimized may have in a setting. At a minimum, TIC services endeavor to do no harm – to avoid retraumatizing or blaming for their efforts to manage their traumatic reactions. It is a philosophical/ cultural stance that integrates awareness and understanding of trauma.
Universal Trauma Precautions (Trauma Awareness)
Since I wrote this original article we have all experienced trauma in some fashion or another due to the coronavirus or the social changes we are experiencing in our country.
- Assume that all people and connected persons with whom you are working are coping with the effects of trauma and modify your practice accordingly.
- Recognizing how your organization, your program, your environment, and your practice could potentially act as a trauma trigger.
- Recognize that you may also have experienced trauma yourself, and you may be triggered by client responses and behavior.
What is an Action Plan we can Embrace as Providers of Care in the Workers’ Compensation Industry?
Six Guiding Principles to a Trauma-Informed Approach
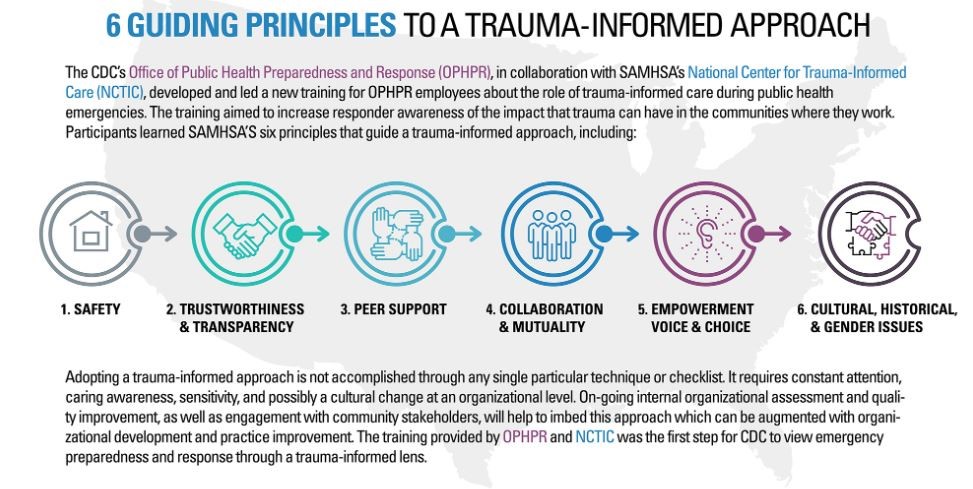
- Safety
- Ensuring physical and emotional safety
- Meeting people where they are
- The person’s culture is respected and incorporated into all stages of intervention
- Identification and on-going assessment of triggers and plans to address these
- Establish and maintain predictable routines to increase the sense of safety
- Maintain a calm environment to decrease hyperarousal
- Support and promote positive and stable relationships in the person’s life
- Ensure opportunities for success
- Trustworthiness
- Maximizing trust through transparency, task clarity, consistency, and interpersonal boundaries
- Provide clear information about when, where, and by whom services will be provided
- Be on time
- Do what you say you will do, and if you can’t do it, take responsibility
- Talk about the good, the bad, and the ugly
- Avoid “tricking” or “catching” people
- Choice
- Maximizing client experiences of choice and control
- When and where will you meet?
- How does the person prefer to communicate?
- How does the person prefer to be addressed?
- Who will be on the team?
- What services does the person want?
- Person decides which goals to work on first
- When does the person want to terminate services?
- Collaboration
- Sharing of power
- Ask about a client’s goals or priorities
- Service plans should be developed by the client, with the support of the case manager
- Ongoing assessment of which services have been effective
- Do goals and service plans need to be adjusted?
- Shared expectations for the helping relationship
- During emotional times ask, “How can I support you right now?”
- Empowerment
- Prioritizing empowerment and skill-building
- Focus on empowerment instead of management and control
- Build upon strengths and promote resilience
- Cultural, Historical and Gender Issues
- The organization moves past cultural stereotypes and biases
- Incorporates policies, protocols and processes that are responsive to the racial, ethnic and cultural needs of individuals served; and recognizes and addresses historical trauma